
Healthcare facility planning requires infrastructure investment decisions that will support strategic choices and operational realities for decades. These investments must perform financially in an uncertain future, and one of the greatest uncertainties is how site-neutral payment policy will impact revenues across different sites of care. Policymakers have pursued such reforms for over a decade, yet only limited changes have been enacted. The most significant effects are still ahead.
For most hospital systems, profitable outpatient procedural services are essential to maintaining systemwide financial viability, but these are the very services most at risk under site-neutral policies. A misalignment of facility assets—for example, hospital operating rooms (ORs) versus ambulatory surgery centers (ASCs)—and payment structure can threaten health system financial viability. Therefore, predicting the impact of site neutrality is critical for planning.
What Is Site Neutrality?
Traditionally, Medicare and other payors pay higher rates when a service is provided in a hospital outpatient department (HOPD) than in a freestanding physician office, even if the service is identical (the rationale is that hospital cost structures are higher and hospitals must offset charity care, etc.). Site-neutral policy aims to remove this difference.
Key Medicare Outpatient Payment Categories Affected by Site-Neutral Policies
For Medicare specifically, it is important to understand the different payment mechanisms for different provider types as discussed below. Commercial payors typically follow Medicare’s payment approach within one or two years.
HOPDs: Paid through the Outpatient Prospective Payment System (OPPS) and can be located either on campus or off campus. Off-campus sites (greater than 250 yards from a hospital building) are called provider-based departments (PBDs). PBDs developed before November 2, 2015 have excepted (or grandfathered) payment status and can retain certain HOPD rates. Newer PBDs (non-excepted) do not qualify for HOPD payments—they are paid under the Medicare Physician Fee Schedule (MPFS). Clinic visits at excepted (grandfathered) PBDs are paid through OPPS at “MPFS-equivalent rates” (40% of OPPS).
Physician & Other Professional Services: Paid through the MPFS. Physician services on hospital campuses currently receive MPFS payments plus hospital facility fees (OPPS). However, CMS requested public comment on whether it should apply site-neutral payments to this group of services as part of the 2026 OPPS/ASC final rule.
ASCs: Medicare-certified ASCs are paid under the ASC fee schedule, which has rates that are typically 30% to 50% lower than OPPS rates but higher than MPFS rates. A hospital-owned surgical center may either be certified as an ASC or an HOPD/PBD, but not both.
How Likely Is CMS to Enact New Site-Neutral Policies?
The push toward site neutrality is accelerating, but not all services or locations will be affected equally or at the same time. For example, lower-acuity services such as clinic visits and drug administration are more likely to be affected, while higher-acuity on-campus services, such as major surgeries, are less likely. Changes to on-campus rates are considered less likely (and more politically difficult) due to the potentially destabilizing effect they would have on vulnerable hospitals, which must subsidize uncompensated care for emergency and other essential services.
Likely Impact on Hospital-Based Services Due to Site-Neutral Policies
| Service Category | Likelihood of Site-Neutral Expansion: Off-Campus (Grandfathered PBDs) | Likelihood of Site-Neutral Expansion: On-Campus HOPDs | Notes/Policy Drivers |
|---|---|---|---|
| Clinic Visits | Very High Already applied to non-excepted sites, likely to extend to excepted | Moderate CMS requested comment in 2026 OPPS rule | Established precedent; MedPAC & CBO cite as top savings source |
| Drug Administration/Infusion | High CY 2026 rule applies PFS rate to excepted off-campus PBDs | Moderate CMS RFI for future inclusion | CMS sees this as the next expansion area (excludes reimbursement for drug costs) |
| Diagnostic Imaging (CT/MRI/Ultrasound) | Moderate | Moderately Low | MedPAC supports; CMS cautious due to access concerns; already partially addressed under imaging caps |
| Diagnostic Testing (Cardiac Echo, Labs, EEGs, etc.) | Moderate | Moderately Low | Low complexity services; may follow imaging reforms in later waves |
| Minor Surgical Procedures (Cataract, Cystoscopy, Arthroscopy, etc.) | Moderate | Moderately Low | Many are ASC eligible; cost differences measurable |
| Major Outpatient Surgery (Total Joint, Spine, Cardiac Cath, etc.) | Moderate | Low | Higher complexity; safety still under study |
| Chemotherapy Services | Moderate | Low | High-cost drugs; political sensitivity; may be delayed |
| Radiation Therapy | Moderate | Low | Likely affected by parallel bundled payment pilots |
When Will Site-Neutral Changes Occur?
One of the most critical and uncertain aspects of site-neutral enactment is timing. Hospitals that transition too fast to non-HOPD locations risk losing 30% to 50% of revenue for key services. Those that move too slowly risk financial losses due to high hospital-based cost structures relative to payment levels.
Understanding likely timing scenarios is critical to projecting financial impact. Policy changes typically occur along one of three paths shown below, based on the financial impact and political complexity of the proposed change. Each path represents a different timeline.
- Fast (CMS rule path; 1 to 3 years): CMS can propose, finalize, and phase in changes via the annual OPPS/ASC rulemaking cycle or separate policy memos. However, CMS is required by law to implement OPPS payment changes on a budget-neutral basis, e.g., increasing rates for some OPPS services to offset reductions in other services. Changes implemented by rule can take effect within one or two years but often face litigation and implementation complexity. This path typically leads to smaller, incremental changes.
- Medium (Congressional targeted law with off-campus focus; 3 to 7 years total): Legislation can take one to three years to pass if attached to a must-pass vehicle or if bipartisan consensus forms. Implementation could be phased over an additional two to four years.
- Slow/Uncertain (broad on-campus parity by statute; 8+ years): Sweeping statutory change to on-campus payments is politically difficult and would likely be phased, contested, include budget-neutral provisions, or include many carveouts. Expect multiyear debate and a multiyear phase-in.
Timing also depends on the location of services. Effects on outpatient services on hospital campuses will take longer than those in grandfathered off-campus locations, as shown below.
Likelihood of Timing for Site-Neutral Policies
| Short-Term (1–3 Years) | Intermediate-Term (3–7 Years) | Long-Term (8+ Years) | |
|---|---|---|---|
| On-Campus Hospital Departments | Unlikely (except physician fees/infusion) | Moderately Unlikely (especially high-acuity procedural services) | More Likely (over time, especially >10 years) |
| Off-Campus Grandfathered Sites | Moderately Likely | Likely (most services) | Highly Likely (all services) |
How Much Will Site-Neutral Policies Affect Hospital Revenues?
Site-neutral policies have consistently sought to lower hospital payment rates to eliminate payment gaps between sites of care. Estimated payment gaps differ by service as summarized below.
Medicare Payment Gap by Service Category
| Service Category | Estimated Payment Gap (vs. ASC/MPFS)* |
|---|---|
| Clinic Visits | 60–70% |
| Drug Administration/Infusion | 40–60% |
| Diagnostic Imaging (CT/MRI/Ultrasound) | 35–55% |
| Diagnostic Testing (Cardiac Echo, Labs, EEGs, etc.) | 25–40% |
| Minor Surgical Procedures (Cataract, Cystoscopy, Arthroscopy, etc.) | 30–50% |
| Major Outpatient Surgery (Total Joint, Spine, Cardiac Cath, etc.) | 30–40% |
| Chemotherapy Services | 30–45% |
| Radiation Therapy | 25–40% |
*Payment gaps vary by billing code. These estimated ranges reflect broad averages for common categories of service.
Rate reductions at these levels would leave many on-campus hospital outpatient services unprofitable, and by extension, negatively affect overall hospital performance. The magnitude of the potential financial impact makes full site neutrality for on-campus services politically unlikely in the short term.
Putting It All Together: Evaluating Payment Scenarios & Facility Master Plan Options
With so many uncertainties surrounding site-neutral payment changes, we encourage organizations to evaluate facility plan options by creating alternate payment scenarios and testing their financial impact on the facility plan options, as shown in the following case study.
This example involves a campus master plan for a replacement hospital. The board of directors was unwilling to invest in the new facility until they understood whether the best investment was to:
- Replace all ORs in the main hospital, or
- Relocate a portion (25%) of ORs to an ASC in anticipation of site-neutral payment policies for surgery.
The organization tested these two facility options against the three payment scenarios shown below to understand the financial impact of each.
Case Study: Facility & Payment Scenario Options for Replacement Hospital Master Plan
| Payment Scenario | Description |
|---|---|
| A. Current Payment Structure | No change in payment structure |
| B. Moderate Site Neutrality | On-campus site neutrality with low commercial payor uptake or CMS budget-neutral policy: begins 2031 |
| C. Full Site Neutrality | Full on-campus site neutrality with high commercial payor uptake: begins 2031 |
| Facility Option | Capital Costs |
|---|---|
| 1. All Hospital ORs | $1.3 billion |
| 2. Shift 25% of ORs to ASC | $1.2 billion |
Case Study: Financial Evaluation of Facility Options Under Site Neutrality Scenarios
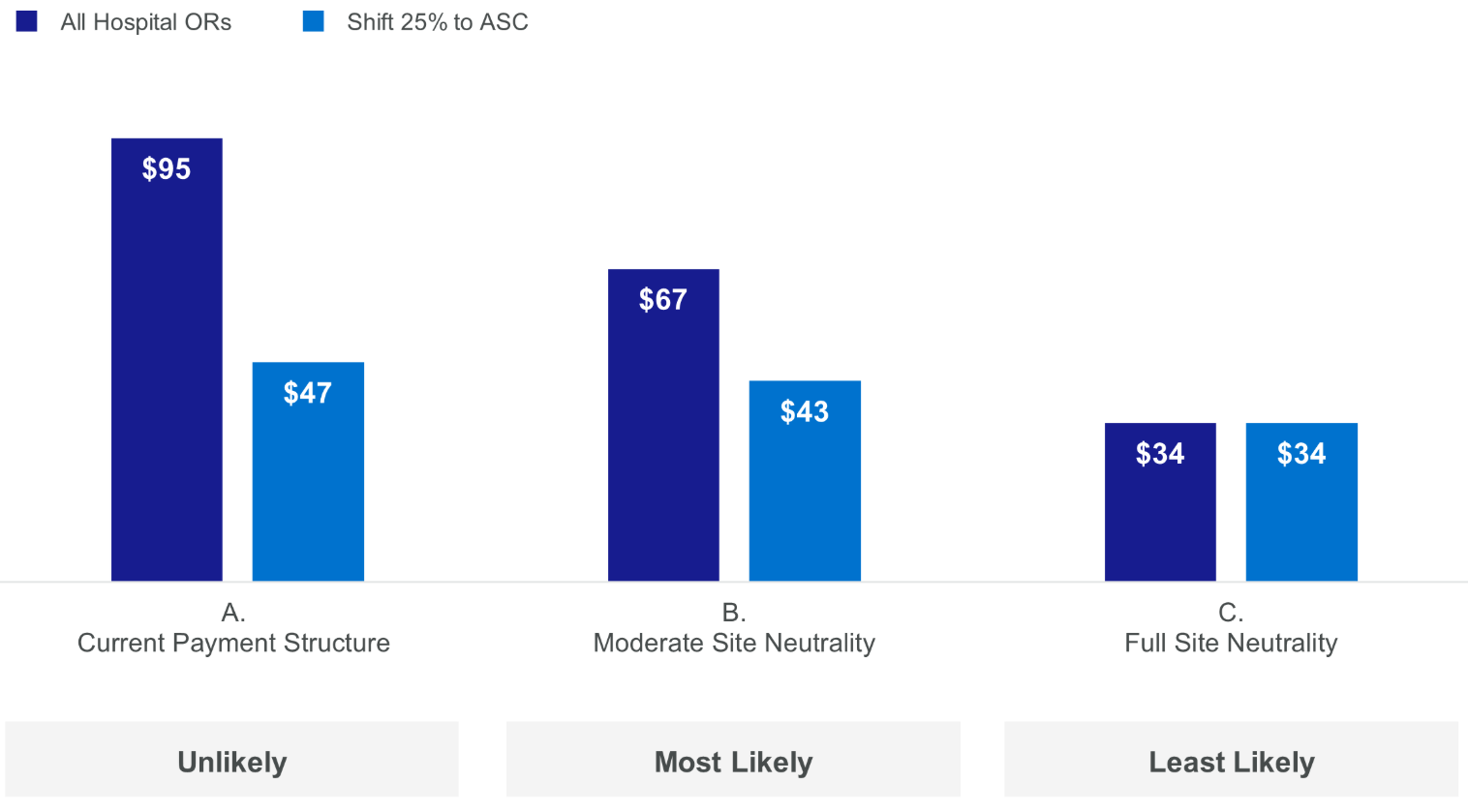
System EBITDA (2035) Under Site Neutrality Scenarios ($M)
Project NPV Under Site Neutrality Scenarios ($M)
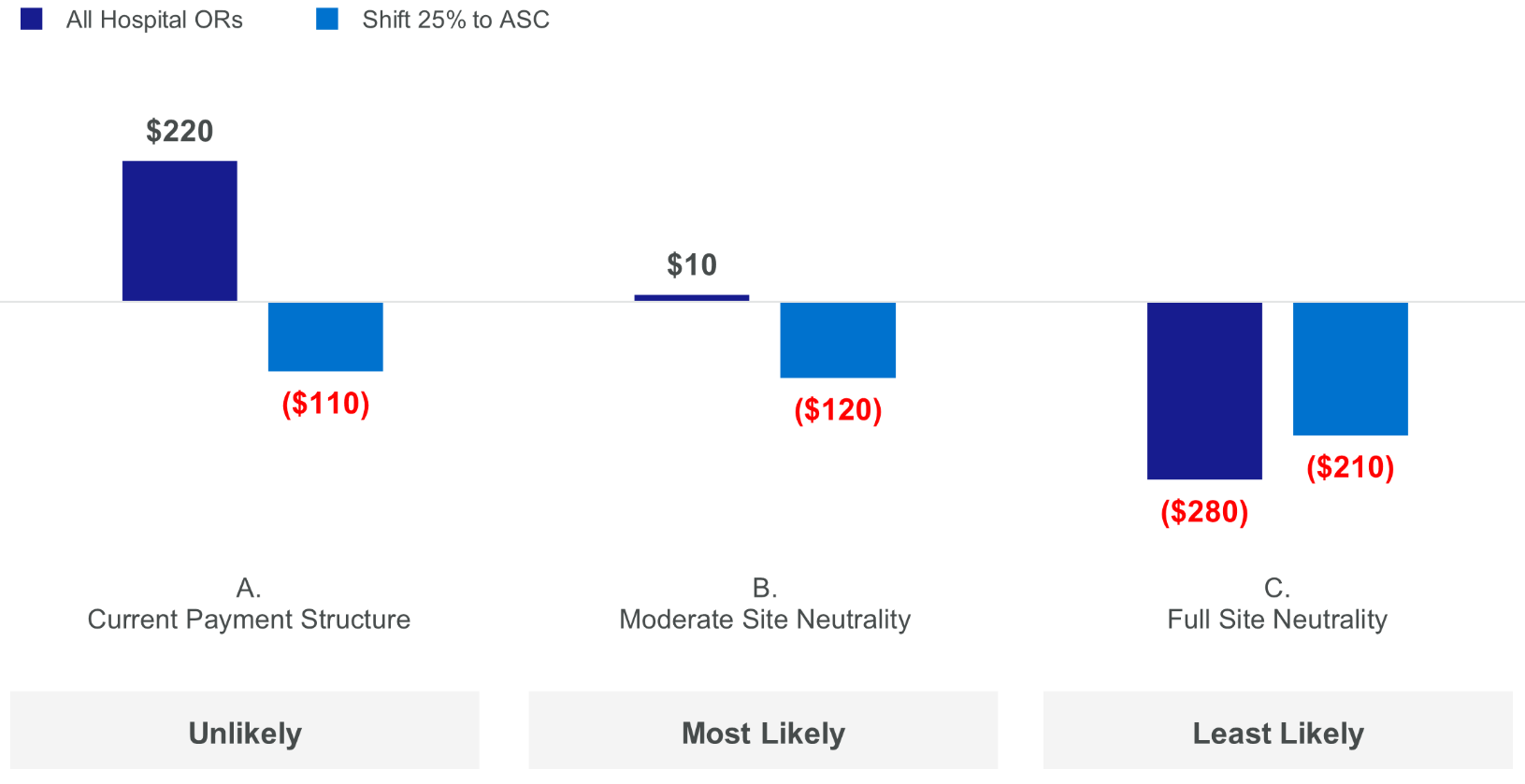
In considering the results, the group believed that the Moderate Site Neutrality scenario (B) was the most likely and the Full Site Neutrality scenario (C) was the least likely during the 10-year planning horizon due to the extreme effect it would have on all hospitals generally.
As shown in the chart above, total system earnings before interest, taxes, depreciation, and amortization (EBITDA) would be cut in half if the system pushed 25% of outpatient surgeries to an ASC while full HOPD rates were still in effect. Based on these results, the group favored the option to keep all ORs in the hospital because it generated the most positive results under the two most likely scenarios. Additional ASC growth could always be considered in future planning phases.
How Forvis Mazars Can Help
Given the stakes associated with site neutrality provisions, it is critical that hospitals and health systems consider their financial impact when determining how outpatient services should be distributed between on-campus and off-campus facilities. At Forvis Mazars, our team has extensive experience assisting organizations with strategic facility and capital planning that considers regulatory and market changes. If you have questions about the effects of site neutrality provisions or would like assistance, please reach out to our team today.